Diabetes and Driving: Rules for Diabetic Drivers
Most diabetics can drive — but you need to monitor blood sugar and know the rules. Hypoglycemia risks, license conditions, and what to do at checkpoints.
There are over 900,000 diabetics living in Czechia. The vast majority of them drive every day without any problems. But one bad day — low blood sugar, a skipped snack, stress at work — and you've got a driver behind the wheel who reacts slower than someone who's been drinking. In the Nový Jičín region, a sixty-year-old man drove 15 kilometers on the wrong side of a busy highway. The cause? Hypoglycemic shock. He didn't kill anyone, but he could have.
This isn't fearmongering. The Immortal study showed that diabetics have double the risk of a traffic accident compared to healthy drivers. Over 40% of accidents involving diabetic drivers are caused by "insufficient attention" or "failure to maintain safe distance" — classic signs of low blood sugar that the driver doesn't even notice.
The good news? Diabetes alone doesn't mean the end of driving. Most diabetics can drive completely legally. But you need to know the rules, monitor your blood sugar, and take it seriously. This article tells you exactly what, when, and how.
Quick summary:
- Diabetes alone does not disqualify you from driving — most diabetics can drive
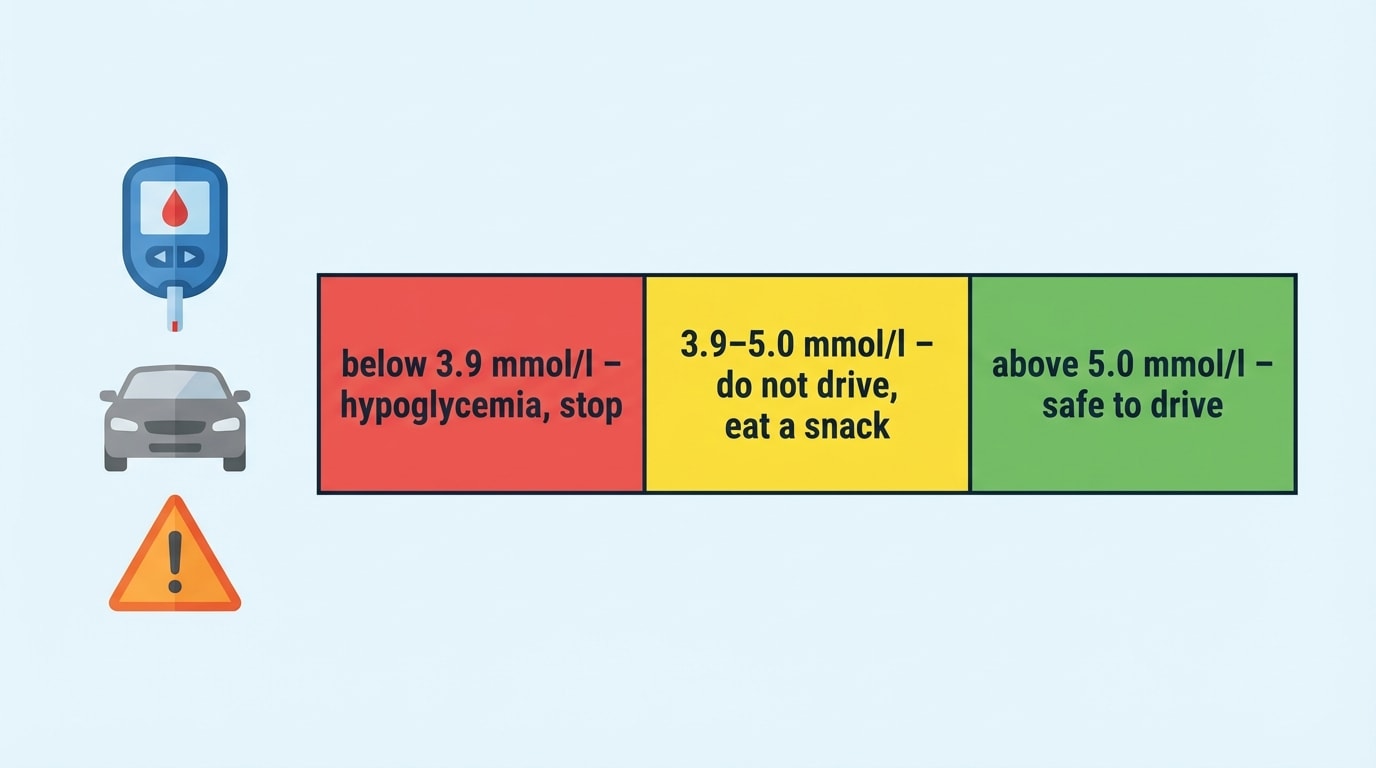
- The key risk is hypoglycemia (blood sugar dropping below 3.9 mmol/l) — don't drive below 5.0 mmol/l
- Two severe hypoglycemic episodes within 12 months = mandatory specialist examination (group 1) or automatic disqualification (group 2)
- Check your blood sugar before every drive — no exceptions
What the Law Says — Diabetes and Your License
The law takes a pragmatic view of diabetes. The disease itself won't cost you your license. What can cost you your license is uncontrolled hypoglycemia — a state where your blood sugar drops so low that you stop functioning normally.
The legal basis is in Decree 277/2004 Coll., specifically in Appendix 3. It defines diabetes mellitus as a condition that may exclude or condition fitness to drive. The key word is "may" — it doesn't automatically mean "excludes." Each case is assessed individually by a doctor.
Amendment 445/2024 Coll. (effective January 1, 2025) confirms the ongoing trend: legislation is moving from blanket restrictions toward individual assessment. The emphasis is on whether the diabetic can demonstrate they manage their condition — monitoring blood sugar, recognizing hypoglycemia symptoms, and knowing what to do.
The doctor has three options when assessing you: fit to drive without restrictions, fit to drive with conditions (such as more frequent check-ups), or unfit to drive. The third option only comes into play with repeated severe hypoglycemic episodes or serious diabetic complications.
What is severe hypoglycemia?
Severe hypoglycemia is a state where you need someone else's help to recover — you can't manage it on your own. This is the key legal criterion. An ordinary hypo that you fix with glucose tablets doesn't count. What matters is whether you needed external assistance.
Group 1 vs. Group 2 — The Key Difference
Just like with epilepsy or heart disease, what matters with diabetes is what type of license you hold. The law distinguishes two groups — and the rules differ dramatically.
Group 1 includes license categories AM, A1, A2, A, B1, B, and B+E. You're in this group if you drive a car, motorcycle, or their trailers — essentially driving for personal use. The rules are more lenient because you drive for shorter periods and without responsibility for passengers.
With group 1, diabetes alone does not disqualify you. Problems arise with repeated severe hypoglycemic episodes. If you have a second (or subsequent) severe hypoglycemic episode within 12 months — meaning you needed another person's help — you must undergo a specialist examination by a diabetologist. They'll decide whether you can continue driving. Important: two severe hypos don't automatically mean losing your license. It depends on the specialist's assessment. Mandatory fitness checks take place at least once every 3 years.
Group 2 includes license categories C1, C, D, and their trailer combinations. This covers professional truck drivers, bus drivers, drivers by profession, and driving school instructors. The rules here are significantly stricter.
With group 2, a second severe hypoglycemic episode within 12 months means automatic disqualification — no "it depends on the assessment." And the conditions for keeping your license are tough. You must prove you've had no severe hypoglycemic episodes in the past 12 months. You must recognize hypoglycemia symptoms. You must measure blood sugar at least twice daily. You must demonstrate sufficient knowledge of hypoglycemia risks. And you must have no diabetic complications. Mandatory checks take place every year.
Diabetes and Driving — Group 1 vs. Group 2
| Criterion | Group 1 (personal) | Group 2 (professional) |
|---|---|---|
| Does diabetes disqualify? | No — not by itself | No — but stricter conditions |
| 2nd severe hypo in 12 months | Mandatory diabetologist exam | Automatic disqualification |
| Unable to recognize hypo symptoms | Mandatory examination | Automatic disqualification |
| Blood sugar monitoring | Before driving (recommended) | At least 2× daily (required) |
| Diabetic complications | Individual assessment | Must have none |
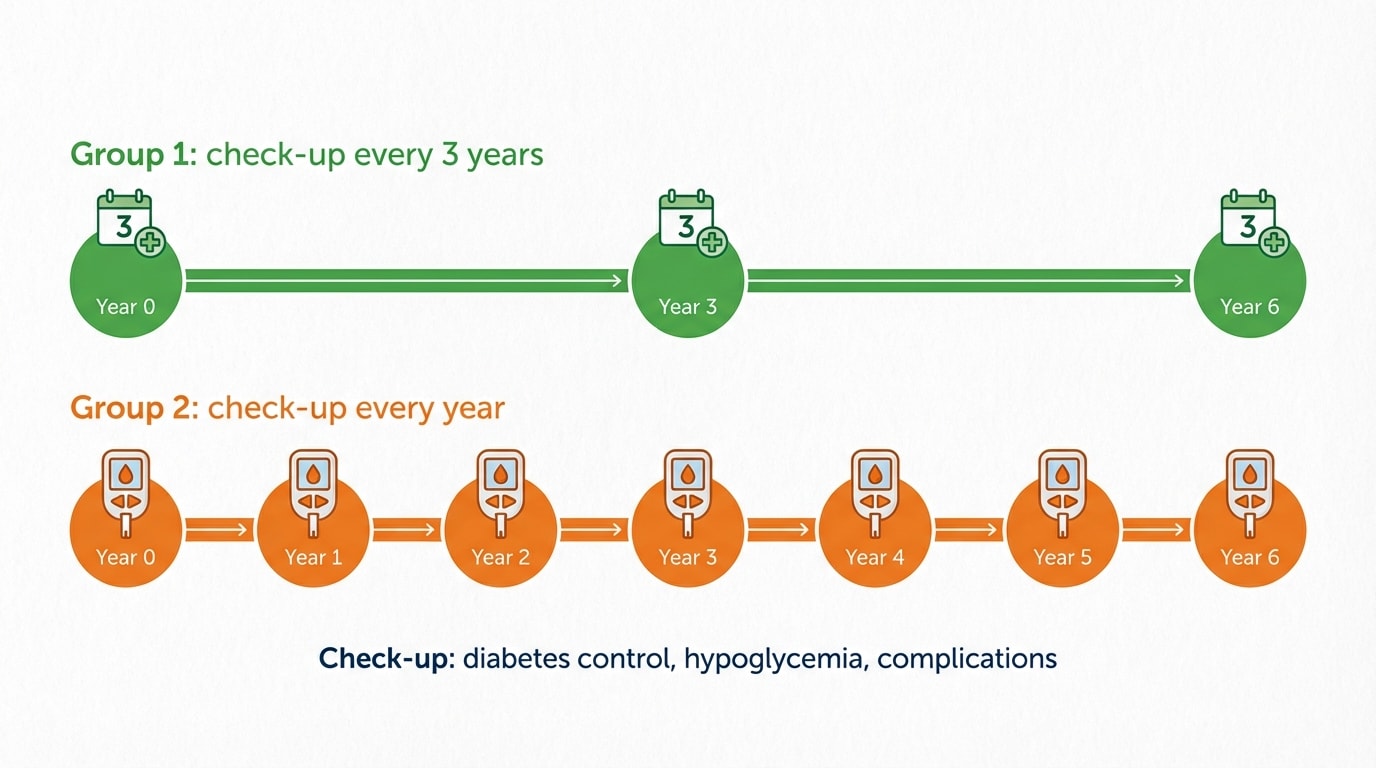
| Check-up frequency | At least once every 3 years | At least once a year |
Hypoglycemia Behind the Wheel — Why It's So Dangerous
Driving is more metabolically demanding than you think. Glucose consumption while driving is up to 17% higher than during regular activities. Your brain works at full capacity while driving — evaluating traffic situations, reacting to stimuli, coordinating movements. And the brain is the first organ that stops working without glucose.
Normal blood sugar levels range between 3.5 and 5.6 mmol/l. Hypoglycemia begins when levels drop below 3.9 mmol/l. But here's the catch — impaired driving ability can occur below 4.5 mmol/l. That's why the safe level for driving is above 5.0 mmol/l. Some sources cite 4.8 mmol/l, but it's better to have a margin.
The symptoms of low blood sugar while driving creep in gradually. It starts with nervousness, pounding heart, and feeling hungry. Then comes sweating, blurred vision, and slowed reactions. In advanced stages, the driver doesn't notice they're drifting out of their lane, braking inadequately, or reacting with delay. In the worst case, unconsciousness sets in — and that's when the car drives itself.
What makes hypoglycemia treacherous is that the driver may not even realize it's happening. There's a condition called "hypoglycemia unawareness." You don't get the warning signals — no pounding heart, no sweating — and you skip straight to the stage where your brain isn't working properly. Under the decree, this is an automatic reason for specialist examination (group 1) or disqualification (group 2).
Don't drive below 5.0 mmol/l
Even though hypoglycemia officially begins below 3.9 mmol/l, driving impairment can start below 4.5 mmol/l. That's why the safe level for driving is above 5.0 mmol/l. Check your blood sugar before every drive — and if it's below 5.0, don't get behind the wheel. Eat a snack, wait, and recheck.
How to Prepare for Driving — A Practical Guide
Print this out and put it in your glove compartment. It's not complicated, but it could save your license and your life.
Before every drive, check your blood sugar with a glucometer. No exceptions — not even for a trip to the corner store. If your level is below 5.0 mmol/l, don't get behind the wheel. Eat something with fast-acting carbohydrates (glucose tablets, a sweet drink, grape sugar), wait 15–20 minutes, and recheck. Below 4.0 mmol/l — absolutely do not drive.
Always keep in your car: a glucometer and test strips, fast-acting carbohydrates (glucose tablets, grape sugar, sweet juice — not chocolate, as it works too slowly), and your diabetologist's contact information. Some doctors also recommend a glucagon injection in case you can't swallow.
On longer trips, check your blood sugar every two hours. Stopping at a gas station? Use it to measure. If your readings are stable, once every two hours is fine. If they're fluctuating, check more often.
If you feel symptoms of hypoglycemia while driving — nervousness, sweating, blurred vision, feeling hungry — pull over immediately and safely. Not "I'll make it to that bend" or "there's a parking lot soon." Stop now, wherever it's safe. Eat 10–40 grams of fast-acting carbohydrates. And here's the crucial point: wait at least 45 minutes before starting the engine again. Recheck your blood sugar. If it's above 5.0 mmol/l and you feel fine, you can continue. If not, call someone to pick you up.
Travel with an informed passenger when possible. A passenger who knows about your diabetes and knows what to do during a hypo (where your sugar is, how to recognize symptoms) is the best insurance you can have.

CGM Sensors — Technology That Helps (But Doesn't Replace a Glucometer)
Continuous glucose monitoring (CGM) has changed many diabetics' lives. Sensors like Dexcom, Medtronic Guardian, and FreeStyle Libre measure blood sugar continuously and can alert you with an alarm when levels are dropping. CGM with alarms can reduce severe hypoglycemic episodes by up to 60%. That's a huge number.
But there's a catch that rarely gets discussed. CGM sensors measure glucose in subcutaneous tissue, not directly in the blood. The data has a delay of 10 to 20 minutes compared to a glucometer — occasionally up to 30 minutes. This means when your CGM shows 5.5 mmol/l, you might actually be at 4.2 mmol/l. During rapid drops, the difference can be even greater.
That's why the rule is clear: CGM is a great supplement, but before driving, rely on your glucometer. If your CGM alarm goes off while driving, pull over and verify the reading with a glucometer. CGM doesn't yet have a special legal status in Czech legislation — the law doesn't mention it as a replacement for standard measurement.
On the other hand, CGM records can play a role in fitness assessments. If your diabetologist sees stable values and infrequent hypoglycemic episodes on your CGM data, it can be an argument in your favor. Technology is evolving fast, and it's likely that legislation will respond over time.
CGM as a helper, not a replacement
CGM sensors have a 10–20 minute delay compared to a glucometer. Always measure with a glucometer before driving. But CGM with alarms significantly reduces the risk of unexpected hypoglycemia — use it as your second line of defense.
Doctor's Reporting Obligation — What Happens Behind Closed Doors
This is the topic that stresses many diabetics more than the disease itself. Fear of losing their license leads some patients to hide hypoglycemic episodes from their doctor. That's understandable, but dangerous — for you and for others.
The law (§86 of Act 361/2000 Coll.) is clear: any doctor — not just a diabetologist, but also a GP, ophthalmologist, or paramedic — who suspects a patient is unfit to drive is obligated to report it to the relevant municipal authority. The doctor doesn't revoke your license — they report their findings to the authority, which then initiates administrative proceedings.
In practice with diabetes, it works like this: your diabetologist discovers repeated severe hypoglycemic episodes during a check-up, inability to recognize symptoms, or serious complications (retinopathy, neuropathy). They inform you — and then inform the authority. For professional drivers, they also notify the employer.
An interesting paradox: modern technology can inadvertently reveal problems you might have been able to hide before. CGM records, insulin pump data, or ambulance records of hypoglycemic episodes — all of this can be part of your medical file that the doctor has access to. Hiding hypoglycemic episodes is therefore not only dangerous but increasingly difficult.
Don't let this scare you, though. One severe hypoglycemic episode in group 1 doesn't mean the end. It means a specialist examination where the diabetologist assesses your overall condition — and most people pass. Details on what to do if your fitness is revoked can be found in the chapter How to Get Your Fitness Back.
Diabetes and Medical Exams — How Often and What to Expect
Diabetics must undergo regular fitness-to-drive checks — but how often depends on your group.
For group 1 (personal drivers), mandatory checks are at least once every 3 years. Your diabetologist assesses whether your diabetes is under control, whether complications have appeared, and whether you recognize hypoglycemia symptoms. Your GP then issues the fitness certificate based on the diabetologist's report.
For group 2 (professional drivers), checks are mandatory every year. Requirements are stricter — besides the diabetologist's report, you must demonstrate regular blood sugar monitoring (at least twice daily), no severe hypoglycemic episodes in the past 12 months, and no diabetic complications. Details about how the medical examination works can be found in the chapter Medical Exam for Driving License.
From January 1, 2026, doctors record certificates electronically in a central database. You don't need to carry the certificate with you — police can verify it in the system. However, older certificates (issued before 2026) must still be carried physically.
Myths About Diabetes and Driving
There are plenty of half-truths circulating about diabetes and driving licenses. Let's debunk the most common ones.
"Diabetics can't drive." False. The vast majority of diabetics can drive. Diabetes alone is not a reason to revoke a driving license. Problems only arise with repeated severe hypoglycemic episodes or serious complications.
"Checking blood sugar in the morning is enough." False. You need to check before every drive. Blood sugar changes throughout the day — you might have 6.0 in the morning and 3.5 in the afternoon. That morning reading is useless in the afternoon.
"After one hypoglycemic episode, I'll lose my license." False. In group 1, one severe hypoglycemic episode doesn't mean automatic revocation. It means a specialist examination by a diabetologist who assesses your overall condition. Only a second severe episode within 12 months leads to more serious measures.
"CGM replaces the glucometer." False. CGM is a great helper, but it has a 10–20 minute delay. Always rely on a glucometer before driving. Use CGM as an early warning system, not your primary measurement.
"In Czechia, diabetics have a special code on their license." False. Unlike Slovakia, where diabetic drivers have code 500 on their license, no special designation exists in Czechia. You're not even required to carry a medical certificate — but diabetologists recommend it, especially for longer trips.
Diabetic Complications and Driving
Diabetes isn't just about blood sugar. Long-term poorly controlled diabetes can lead to complications that affect driving ability — even without hypoglycemia.
Diabetic retinopathy affects nearly 12% of treated diabetics. It's damage to the retina that gradually worsens vision. In advanced stages, it can lead to loss of peripheral vision or even blindness. If you have diabetes, keep up with regular eye exams — not just for driving, but for yourself. Details about vision requirements for drivers can be found in the chapter Vision Disorders and Driving.
Diabetic neuropathy (nerve damage) can cause loss of sensation in your feet — and that's a problem for operating pedals. If you can't feel how hard you're pressing the brake or accelerator, driving becomes dangerous.
Diabetic foot affects about 5.6% of diabetics and in severe cases can lead to amputation, which directly affects fitness to drive.
All these complications are assessed individually by the doctor. None of them automatically means the end of driving — but they can lead to conditional fitness or a requirement for vehicle modifications.
Diabetes Medications and Driving
Not all diabetes medications are equal when it comes to driving. Some can cause hypoglycemia, others can't — and that difference is crucial.
Insulin is the riskiest because it can cause hypoglycemia at any time. Drivers on insulin need to be particularly careful about checking blood sugar before driving and during longer trips.
Sulfonylureas and glinides (drugs that stimulate the pancreas to produce insulin) can also cause hypoglycemia — less frequently than insulin, but the risk exists.
Metformin, GLP-1 agonists, and SGLT-2 inhibitors virtually don't cause hypoglycemia when dosed correctly. If you only take these medications, the risk of hypoglycemia behind the wheel is minimal.
If you take medications that can cause hypoglycemia, all the rules about checking blood sugar before driving apply doubly. More about how specific medications affect driving can be found in the chapter Medications and Driving.
Ask your diabetologist
Whenever your medications change, ask your doctor whether the new medication can cause hypoglycemia and how it affects driving. This is especially important when switching to insulin or sulfonylureas — it may also change your obligation to check blood sugar before driving.
What's New — Recent Changes
Amendment 445/2024 Coll. (effective January 1, 2025) overhauled Appendix 3 of Decree 277/2004 Coll. The main goal: eliminate discrimination against people with health conditions and account for medical progress. The amendment implements EU Directive 2016/1106 and shifts the approach from blanket restrictions to individual assessment.
The basic framework for diabetics — severe hypoglycemia as the key criterion — remains unchanged. But the trend is clear: legislation is gradually recognizing that a diabetic with a sensor, insulin pump, and regular check-ups is a safer driver than many healthy people who drive while fatigued or under the influence of alcohol.
From January 1, 2026, the age threshold for mandatory medical exams also shifted from 65 to 70. If you're a diabetic over 65, you don't need to go for a mandatory exam until you turn 70 — unless your doctor determines otherwise.
Summary
- Diabetes alone does not disqualify you from driving — most of Czechia's 900,000+ diabetics can drive legally
- The key risk is hypoglycemia — don't drive below 5.0 mmol/l, check with a glucometer before every drive
- Group 1 (personal drivers): two severe hypos in 12 months = mandatory examination, checks every 3 years
- Group 2 (professionals): two severe hypos in 12 months = automatic disqualification, checks every year
- CGM is a great helper but has a 10–20 minute delay — don't rely on it alone
- Doctors must report unfitness to authorities (§86) — but one severe hypo doesn't mean the end
- Always keep a glucometer, fast-acting carbs, and your doctor's contact in your car
Key Terms
| Term | Explanation |
|---|---|
| Hypoglycemia | A drop in blood glucose below 3.9 mmol/l. Can cause slowed reactions, blurred vision, and in severe cases, unconsciousness. |
| Severe hypoglycemia | A state where you need someone else's help to recover. Key legal criterion — two severe hypos in 12 months have automatic consequences for group 2. |
| Blood sugar (glycemia) | The level of glucose in the blood, measured in mmol/l. Must be above 5.0 mmol/l for safe driving. |
| CGM (continuous glucose monitoring) | A subcutaneous sensor that continuously measures blood sugar. Has a 10–20 minute delay compared to a glucometer. |
| Group 1 | Non-professional drivers (AM, A, B) — more lenient conditions, checks every 3 years. |
| Group 2 | Professional drivers (C, D) — stricter conditions, annual checks, blood sugar monitoring at least 2× daily. |
| Diabetic retinopathy | Retinal damage caused by diabetes — affects ~12% of diabetics. Can affect fitness to drive. |
| Hypoglycemia unawareness | A condition where the diabetic doesn't get warning signals (pounding heart, sweating) and skips straight to advanced hypo stages. Grounds for specialist examination (group 1) or disqualification (group 2). |
| Decree 277/2004 Coll. | Implementing regulation on medical fitness to drive. Appendix 3 contains conditions for diabetics. |
| §86 of Act 361/2000 | Doctor's reporting obligation — must report driver unfitness to the municipal authority. |