Heart Disease and Driving: After a Heart Attack
After a heart attack, with arrhythmia or a pacemaker — when can you drive again? Waiting periods, conditions for group 1 and 2, and 2025 updates.
Three million Czechs live with cardiovascular disease. And most of them drive. If you're one of them — or your doctor just gave you a diagnosis that left you wondering whether you can still get behind the wheel — read on. Because in most cases, the answer is: yes, you can drive. But you need to meet clear conditions and observe the required waiting periods.
Heart disease doesn't automatically mean the end of your driving days. Heart attack, arrhythmia, pacemaker — these are all conditions that thousands of drivers recover from every year and return to driving. The key is knowing exactly what the law requires, how long you need to wait, and what examinations you need. This article gives you concrete answers — waiting periods for specific events, differences between regular and professional drivers, and the process for getting back behind the wheel.
Quick summary:
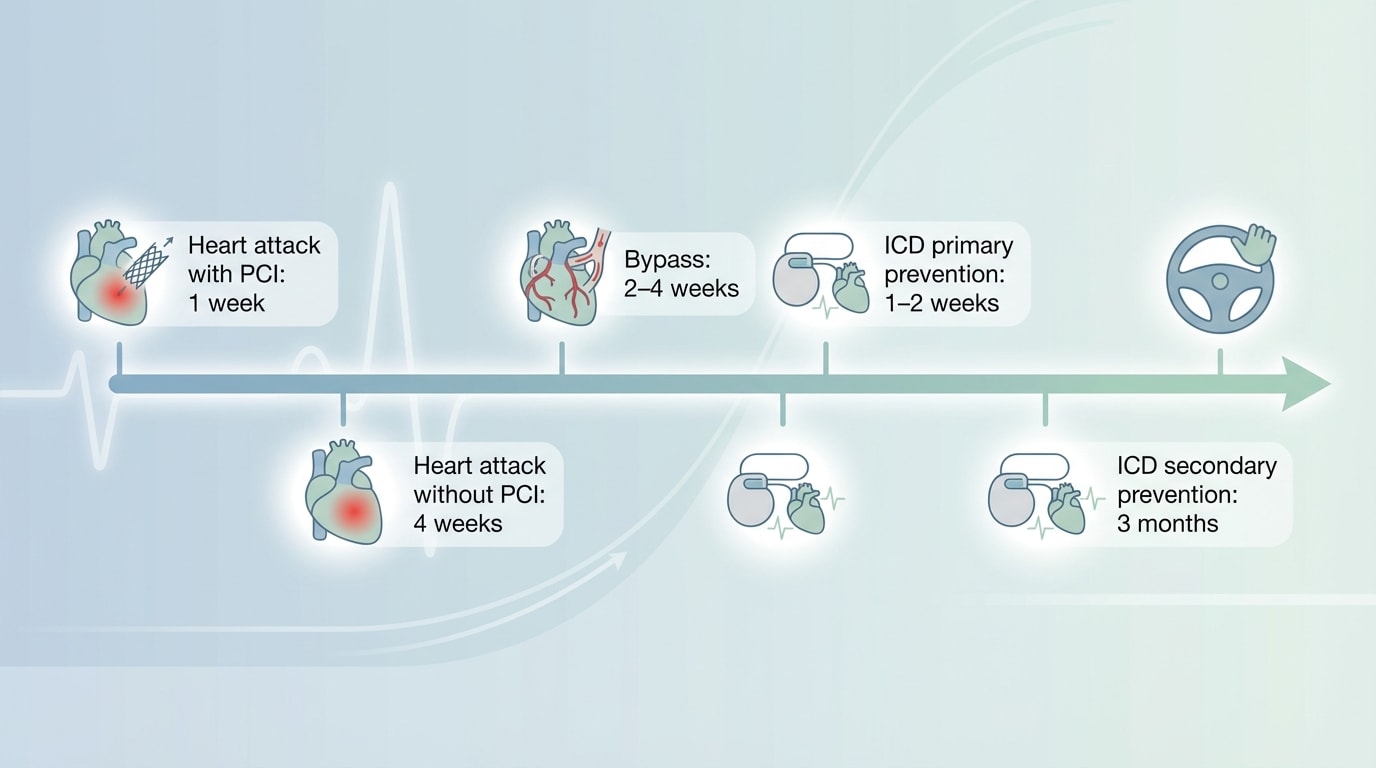
- After a heart attack with successful stenting and EF > 40%, you can drive after just 1 week (group 1)
- A pacemaker usually means no restrictions for regular drivers
- An implanted defibrillator (ICD) permanently disqualifies you from driving trucks and buses (group 2)
- From January 2025, amendment 445/2024 Coll. adds new diagnoses — Brugada syndrome, arrhythmogenic cardiomyopathy, and malignant hypertension
What the Law Says — Two Groups, Two Standards
Just like with vision disorders or epilepsy, Czech legislation distinguishes two groups of drivers — and the requirements differ dramatically.
Group 1 includes non-professional drivers with categories AM, A1, A2, A, B, and B+E. Here, the law is relatively accommodating. Most heart conditions won't permanently disqualify you. After a heart attack, after stenting, with a pacemaker — you just need to observe the waiting period, pass a cardiology examination, and get a positive assessment.
Group 2 includes professional drivers — categories C, C+E, D, D+E, and professional drivers by occupation. This is a different world. The law is stricter, waiting periods are longer, and some conditions disqualify you from professional driving entirely. The logic is simple: a truck or bus driver has tons of cargo or dozens of people behind them. A sudden loss of consciousness at the wheel would have catastrophic consequences.
Remember the key difference when it comes to implanted defibrillators (ICD). A regular driver with an ICD can drive a car after the waiting period. A professional driver with an ICD must never drive a truck or bus — ever. It's a permanent contraindication for group 2.
The legal basis is found in Decree No. 277/2004 Coll., specifically in Annex 3, Chapter IV (circulatory system). It distinguishes two sections: conditions excluding fitness (absolute ban) and conditions requiring specialist assessment (driving permitted after examination).
After a Heart Attack — When Can You Drive Again
A heart attack is a shock for most people. And one of the first questions you'll ask after stabilization is: "Will I still be able to drive?" Good news: in most cases, yes. And sooner than you might expect.
If doctors performed a successful percutaneous coronary intervention (PCI — in practice, this means they inserted a stent into a narrowed artery) and your left ventricular ejection fraction is above 40%, you can get behind the wheel after just one week. The ejection fraction is a number that tells you how well your heart pumps blood — above 40% means the heart is working adequately. Your cardiologist will tell you the result after an echocardiogram.
If the PCI wasn't successful or your ejection fraction dropped below 40%, the waiting period extends to 4 weeks from the event. Even so, it's a relatively short time. After four weeks, the cardiologist will assess your condition, perform a follow-up examination, and decide based on the results.
For professional drivers (group 2), the situation is more demanding. After a heart attack, you must wait at least 6 weeks. And your ejection fraction must be above 35%. If it's lower, you're unfit for professional driving — until your condition improves.
What is ejection fraction (EF)?
Ejection fraction indicates what percentage of blood the heart pushes out with each beat. Normal value is 55–70%. For driving (group 1) you need EF above 40%, for professional driving (group 2) above 35%. It's measured by echocardiography — a standard heart ultrasound.
Bypass, Stents, and Valve Surgery — Waiting Periods
Cardiac surgery doesn't mean the end of your time behind the wheel. But each procedure has its own waiting period — and you must observe it before getting back behind the wheel.
Planned angioplasty (PCI / stenting) — when it's not an acute heart attack but a planned procedure — has the shortest waiting period of all. For group 1, virtually no restrictions after a successful procedure. For group 2, it's 4 weeks with an annual cardiology check-up.
Coronary artery bypass grafting (CABG) is a more invasive procedure. The breastbone is cut and needs time to heal. For group 1, expect 2–4 weeks — depending on how quickly the chest heals and whether you're still taking strong painkillers (which affect your ability to drive — more on that in the chapter Medications and Driving). For group 2, it's 3 months plus a mandatory stress test.
Heart valve surgery — whether replacement or repair — requires at least 4 weeks of recovery for group 1. For professional drivers, the waiting period is determined individually, but typically runs 3 months or more.
After cardiac arrest, the rules are strictest. For group 1, it's a minimum of 3 months with individual assessment by a cardiologist. For group 2, cardiac arrest is generally a permanent contraindication — professional driving after it is usually not possible.

Pacemaker vs. Defibrillator — A Critical Difference
This is where many people get confused. A pacemaker and an implantable cardioverter-defibrillator (ICD) are two completely different devices — and the law treats them very differently.
A pacemaker maintains a regular heart rhythm. It sends small electrical impulses to ensure the heart beats fast enough. For regular drivers (group 1), this means virtually no restriction — at most a week after implantation. Even for professional drivers, the limitation is minimal: 1 week, or 4 weeks if you have a history of fainting or are dependent on the pacemaker. The myth that "you can't drive with a pacemaker" is exactly that — a myth.
An ICD (defibrillator) is a different story. This device doesn't just maintain rhythm — it can deliver a powerful electric shock to stop a life-threatening arrhythmia. And that shock is the problem. Imagine you're driving on the highway and the device suddenly fires — a jolt that knocks you out for a fraction of a second. That's why the rules for ICDs are much stricter.
For group 1, it depends on the reason for implantation. If it's primary prevention (you receive an ICD preventively because you have a high-risk condition but haven't had a serious arrhythmia yet), the waiting period is 1–2 weeks. If it's secondary prevention (you got an ICD after cardiac arrest or a serious arrhythmia), you wait 3 months. And if the ICD delivered an appropriate shock (the device actually intervened), you wait another 3 months from the last event.
For group 2, it's unambiguous: ICD is a permanent contraindication. A truck or bus driver with an implanted defibrillator must never drive professionally — ever. It's one of the few absolute lines in the law. If you're a professional driver and receive an ICD, it means the end of your career behind the wheel of a heavy vehicle. But you can still drive a car (after observing the waiting period).
ICD = end of professional driving
An implantable cardioverter-defibrillator (ICD) permanently disqualifies you from driving group 2 vehicles (trucks, buses). For personal driving (group 1), waiting periods apply: 1–2 weeks (primary prevention) or 3 months (secondary prevention / after a shock). Battery replacement: 1 week.
Arrhythmia and Syncope — When Fainting Becomes a Problem
Arrhythmia — a heart rhythm disorder — is a broad term. Some arrhythmias are harmless and have no effect on driving. Others can cause sudden loss of consciousness (syncope), and that's a catastrophe behind the wheel.
The law draws a simple line: if an arrhythmia causes syncope, you're fit with conditions. You must demonstrate that the condition is under control — through treatment, medication, or an intervention. If the arrhythmia doesn't cause syncope, there's generally no reason for restriction.
Syncope of unknown cause — fainting where doctors can't find a clear reason — has its own rules. If it's a first episode and the cardiologist rules out a cardiac cause, you don't need to worry. For group 1, no restrictions. But if syncope recurs, you wait at least 6 months and the cardiologist must assess your condition individually. For professional drivers, recurrent syncope is generally grounds for permanent unfitness.
From January 2025, amendment 445/2024 Coll. added several diagnoses to the decree that weren't previously explicitly listed: Brugada syndrome with syncope or cardiac arrest in the medical history, arrhythmogenic right ventricular cardiomyopathy, and catecholaminergic polymorphic ventricular tachycardia. If your doctor diagnoses any of these conditions, you now fall under the formal fitness assessment process.
Heart Failure and the NYHA Classification
Heart failure doesn't mean your heart has stopped working. It means it's not pumping blood as efficiently as it should. Doctors classify it into four grades using the NYHA system (New York Heart Association) — and that grade determines whether you can drive.
NYHA I — you have no symptoms during normal activity. You climb stairs, work, exercise without shortness of breath. You're fit to drive with conditions — a specialist cardiology examination is sufficient. Interestingly, amendment 445/2024 originally required a cardiology examination even for NYHA I, which sparked controversy because these patients are asymptomatic and don't regularly visit a cardiologist. The Ministry of Health subsequently issued an interpretive opinion that softened this requirement.
NYHA II — normal activity causes shortness of breath or fatigue, but you're fine at rest. Fit with conditions, same as NYHA I.
NYHA III — even mild exertion causes symptoms. For group 1, you're still fit with conditions, but the assessment is strictly individual. For group 2, you're unfit.
NYHA IV — you have symptoms even at rest. Unfit for both groups. Driving in this condition is dangerous.
For professional drivers with any degree of heart failure, there's an additional requirement: ejection fraction above 35%. If it's lower, group 2 driving isn't possible — regardless of the NYHA grade.
NYHA classification and fitness to drive
| NYHA class | Description | Group 1 (personal) | Group 2 (professional) |
|---|---|---|---|
| I | No limitation during normal activity | Fit with conditions | Fit with conditions (EF > 35%) |
| II | Shortness of breath/fatigue with normal activity | Fit with conditions | Fit with conditions (EF > 35%) |
| III | Symptoms even with mild exertion | Individual assessment | Unfit |
| IV | Symptoms at rest | Unfit | Unfit |
Hypertension — When High Blood Pressure Matters
Hypertension is the most common cardiovascular disease in Czechia — affecting about a third of the adult population. And the vast majority of these people can drive without any issues whatsoever. Uncomplicated hypertension that's treated and well-controlled with medication provides no grounds for any driving restriction.
The problem arises with so-called malignant hypertension. Amendment 445/2024 Coll. defines it as systolic pressure of 180 mmHg or higher, or diastolic of 110 mmHg or higher — combined with imminent or progressive organ damage (heart, kidneys, brain, eyes). Malignant hypertension is now explicitly listed as a condition requiring fitness assessment — meaning you must undergo a specialist examination.
Hypertension accompanied by symptoms — dizziness, fainting, vision problems — also precludes driving until the condition is stabilized. And poorly controlled hypertension with advanced organ damage can exclude fitness entirely.
The practical takeaway: if you take blood pressure medication and your pressure is under control, you have nothing to worry about. Keep attending your check-ups, take your medication consistently, and live normally. But if your readings repeatedly show values above 180/110, take it seriously — not just because of your license, but because of your health.
Your Doctor Must Report You — What Happens After Diagnosis
One thing many drivers don't know: your doctor has a legal obligation to report you. It's not a matter of their goodwill — the law mandates it.
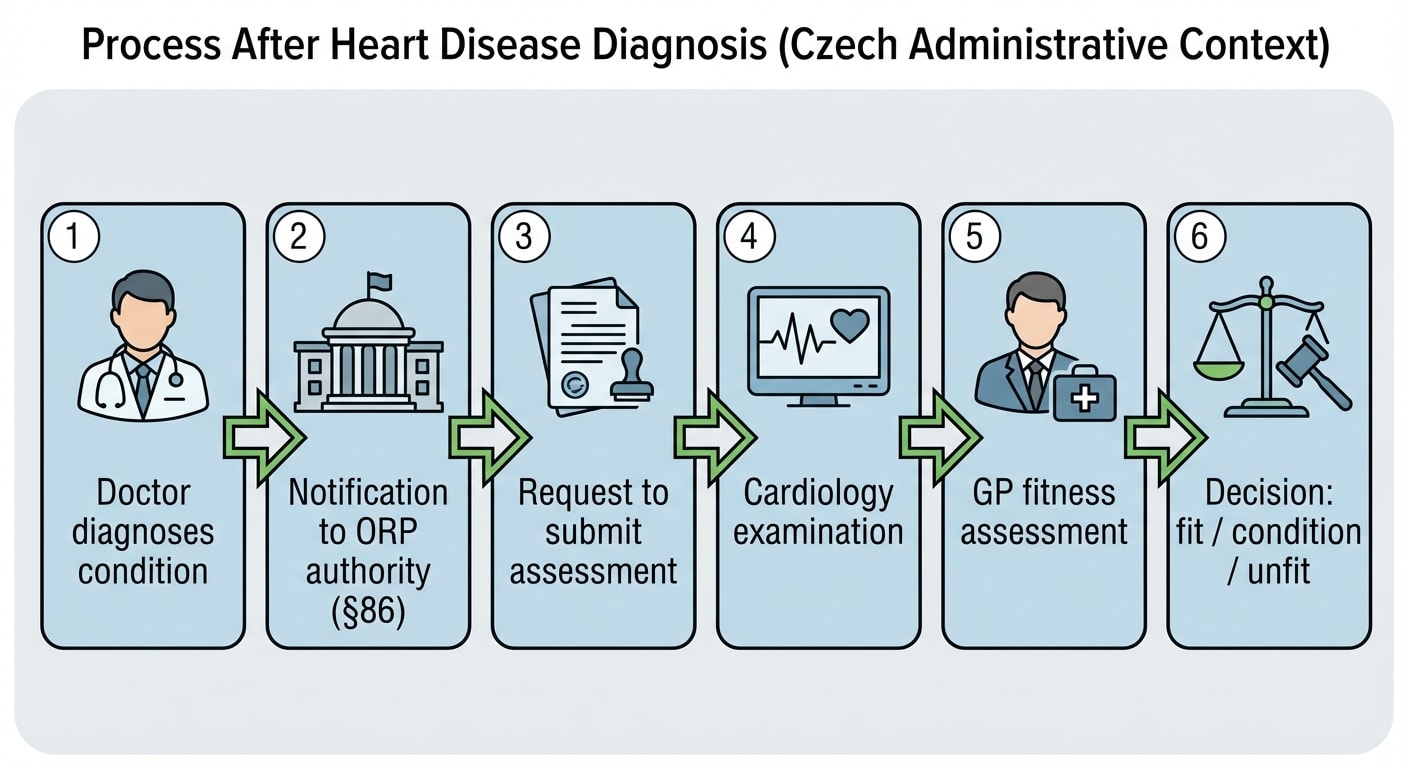
Under §86 of Act No. 361/2000 Coll., every doctor — whether a GP, cardiologist, or other specialist — must immediately notify the municipal authority of the municipality with extended powers (ORP) if they determine that a driver is medically unfit or fit only with conditions. You don't have to be their registered patient. It's enough that they examined you and identified a relevant diagnosis.
What happens next? The authority will request that you submit a current medical assessment. You'll need a cardiology examination — ECG, echocardiography, possibly a stress test. Based on the cardiologist's findings, your GP issues an assessment: fit, fit with conditions, or unfit.
An important point: your license isn't taken away by the doctor. The decision is made by the authority through an administrative procedure. And you can appeal their decision. The entire process is described in detail in the chapter How to Get Your License Back.
You can't hide it
Driving with a health condition that excludes fitness is an offense. If you cause an accident, it's an aggravating circumstance — criminal prosecution is possible. Additionally, your insurance company can refuse to pay out both liability and collision claims.
How Much It Costs and Where to Get Examined
A cardiology examination for your fitness assessment is typically paid out of pocket — insurance only covers it as part of your regular cardiology care. Expect to pay CZK 500–1,500. Echocardiography (heart ultrasound) costs CZK 800–2,000, and a stress test (ergometry) CZK 1,000–2,500. Add the GP's fitness assessment at CZK 400–600 — which insurance doesn't cover and you always pay yourself.
You can get examined by your outpatient cardiologist. If you don't have one, ask your GP for a referral — appointment wait times vary by region, but for assessment examinations you'll usually be seen as a priority. In urgent cases (after an acute event), the cardiology examination will take place while you're still in the hospital, before discharge. Details about the medical examination process can be found in the relevant chapter.
After stabilization, you'll attend regular check-ups. For chronic heart conditions, this is typically once a year — the cardiologist evaluates your condition and renews your assessment.
What Changed in 2025 — Amendment 445/2024
From January 1, 2025, an amendment to Decree No. 277/2004 Coll. (numbered 445/2024 Coll.) took effect, refining and tightening the cardiovascular section. What's new?
New diagnoses — conditions that weren't previously explicitly listed made it into the decree: Brugada syndrome with syncope or cardiac arrest in the medical history, arrhythmogenic right ventricular cardiomyopathy, and catecholaminergic polymorphic ventricular tachycardia. All three are now formally addressed.
Malignant hypertension — newly defined as systolic pressure ≥ 180 mmHg or diastolic ≥ 110 mmHg with organ damage. Previously not explicitly mentioned in the decree.
Carotid stenosis — narrowing of the carotid artery is now explicitly listed as a condition requiring fitness assessment.
Stricter rules for group 2 — structural cardiomyopathies meeting specific criteria (wall thickness, presence of arrhythmia) now exclude professional driving.
Czechia draws on EU Directive 2006/126/EC (Annex III), which harmonizes rules for driving and cardiovascular disease across the EU. Amendment 445/2024 implements these European standards into Czech law.
Myths About Heart Disease and Driving
There are plenty of misconceptions about heart disease and driving. Let's debunk them.
"After a heart attack, I'll never be allowed to drive again." That's not true. Most people return to driving after a heart attack — often within one to four weeks. It depends on the treatment outcome and ejection fraction.
"With a pacemaker, I can't drive." Another myth. A pacemaker means virtually no restrictions for regular drivers. At most a week after implantation — and you're back on the road.
"With a defibrillator, I can drive a truck." Unfortunately, that's not true. An ICD permanently disqualifies you from group 2 driving. Car yes, truck no.
"High blood pressure is just a number." Malignant hypertension with organ damage has been explicitly addressed in the decree since 2025. It's not just a number — it's a health risk that also affects your ability to drive.
Summary
- After a heart attack with PCI and EF > 40%, you can drive after 1 week (group 1); without PCI, after 4 weeks
- Pacemaker = virtually no restrictions for regular drivers
- ICD = permanent contraindication for professional driving (group 2)
- Heart failure NYHA IV = unfit for both groups
- Your doctor must report you to the authority — concealing your condition is an offense
- From 2025, the amendment refines conditions: Brugada syndrome, malignant hypertension, carotid stenosis
- Cardiology examination for assessment: CZK 500–1,500 + GP assessment CZK 400–600
Key Terms
| Term | Explanation |
|---|---|
| Ejection fraction (EF) | The percentage of blood the heart pushes out with each beat. Normal is 55–70%. For group 1 driving, you need EF > 40%; for group 2, > 35%. |
| PCI (percutaneous coronary intervention) | A catheter-based procedure where a stent is inserted into a narrowed coronary artery. After successful PCI with EF > 40%, you can drive after 1 week. |
| CABG (coronary artery bypass grafting) | A surgical procedure that bypasses a narrowed artery using a graft. Waiting period: 2–4 weeks (group 1) or 3 months (group 2). |
| ICD (implantable cardioverter-defibrillator) | A device that monitors heart rhythm and can deliver a shock during a life-threatening arrhythmia. Permanent contraindication for group 2. |
| Pacemaker | A device that maintains regular heart rhythm using electrical impulses. Minimal driving restrictions. |
| NYHA classification | A four-grade system for evaluating heart failure (I–IV). Determines the level of limitation during normal activity and affects driving fitness. |
| Syncope | A sudden, brief loss of consciousness caused by reduced blood flow to the brain. Behind the wheel, it can be fatal. |
| Decree 277/2004 Coll. | Implementing regulation on medical fitness to drive. Annex 3, Chapter IV contains cardiovascular conditions. |
| Amendment 445/2024 Coll. | Amendment to the decree effective from January 1, 2025 — refines the cardiovascular section, adds new diagnoses. |
| §86 of Act 361/2000 Coll. | Doctor's reporting obligation: must notify the ORP municipal authority of a driver's unfitness or conditional fitness. |